Poster: Racial/Ethnic Groups Have Different Clustering of Common Cancer Genes
Authors: Peter Beitsch, MD; Chloe Wernecke; Kelly Bontempo, CGC; Brenna Bentley, CGC; Pat Whitworth, CGC; Rakesh Patel, MD; Richard Reitherman, MD; Mariusz Wirga, MD; Anne Peled, MD; Linda Ann Smith, MD
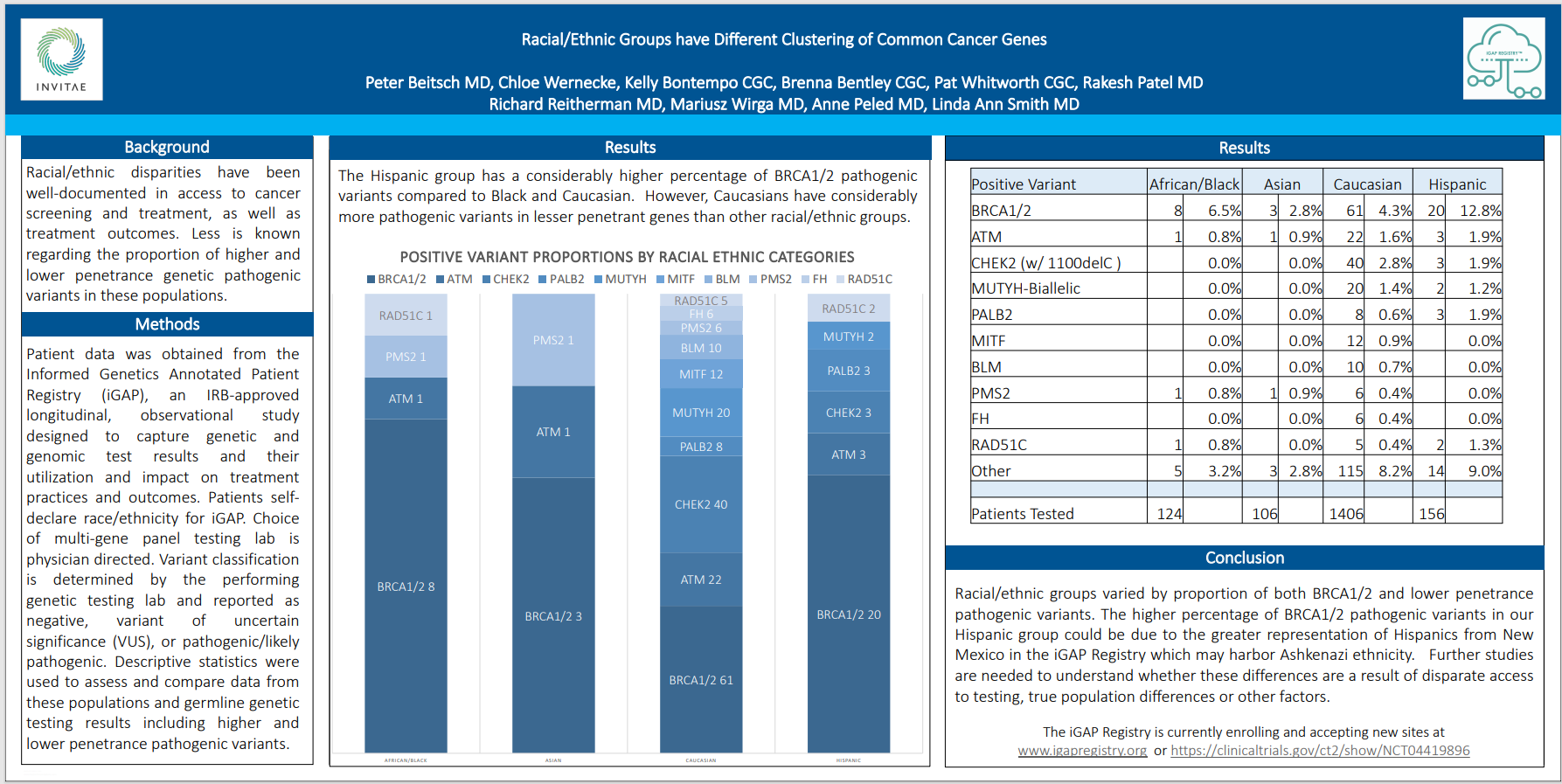
While racial and ethnic disparities in access to cancer screening and treatment have been well documented, less is known about the genetic pathogenic variants across diverse populations and how they might vary. Using data provided by the Informed Genetics Annotated Patient Registry (iGAP), the researchers designed a longitudinal, observational study aimed at capturing genetic and genomic test results, as well as how these results were used, if at all, to influence treatment.
Data on 1,792 patients were reviewed. Of these, 124 were classified as Black or African, 106 were classified as Asian, 156 were classified as Hispanic, and 1,406 were classified as Caucasian. Race and/or ethnicity was self declared by each patient.
Other methods worth noting include these:
- Choice of multi-gene panel testing lab was physician directed
- Variant classification was determined by the genetic testing lab and reported as “negative,” “variant of uncertain significance” (VUS), or “pathogenic/likely pathogenic.”
- Descriptive statistics were used to assess and compare data and germline genetic testing results, including higher and lower penetrance pathogenic variants
The results showed that patients in the Hispanic group had a much higher percentage of BRCA1/2 pathogenic variants than those in the Black/African or Caucasian groups. Caucasians, however, were shown to have considerably more pathogenic variants in lesser penetrant genes than patients of the other racial/ethnic groups.
The researchers make an interesting point in noting that the higher percentage of BRCA1/2 pathogenic variants in the Hispanic group might be due to a greater representation of Hispanics from New Mexico in the iGAP Registry and the possibility that this population is impacted by Ashkenazi ethnicity.
The researchers concluded that further studies are necessary to address remaining questions: For example, are the differences noted a result of disparate access to testing, true populations differences, or some other factor or factors?